Making Every Contact Count – Utilising the Travel Consultation to Increase Hepatitis A Vaccine Coverage Amongst the MSM Community
Paul Costello1, Christopher Ma1, Natalie Vassilouthis1
1Sanofi Pasteur UK & Ireland, Reading, United Kingdom
Download Abstract
Video Summary of Poster
Background
- Recent years have seen hepatitis A outbreaks within the men who have sex with men (MSM) community.1
- Both Public Health England (PHE) and the British Association for Sexual Health and HIV (BASHH) identify MSM as an at-risk group and recommend that vaccination for hepatitis A is offered.2,3
- Travelling to non-endemic countries was implicated in a recent hepatitis A outbreak in the MSM community.
- Between mid-2016 to early-2018, a hepatitis A outbreak affecting the MSM population was reported in the UK and Europe.4
- Whilst hepatitis A infection is not usually life-threatening, hospitalisation and complications can occur.
- Symptoms are generally more common and of greater severity in older people.
Observations
- In non-endemic countries, the risk of hepatitis A from contaminated food is low.
- However, faecal-oral transmission is still possible and remains a risk, especially in certain cohorts, dependent on behaviours. One at-risk cohort is MSM.
- Three hepatitis A virus genotype IA strains relating to the 2016-2018 outbreak were identified:
- VRD_521_2016 (first reported in Netherlands, October 2016).
- RIVM-HAV16-090 (first reported in England, December 2016).
- V16-25801 (first reported in Germany, January 2017).
- In October 2016, the European Union Early Warning and Response System reported two MSM cases with a specific strain of hepatitis A virus.5,6
- The initial infections were traced back to EuroPride in Amsterdam in July/August 2016.
- By 26th June 2017, thirteen EU Member States had reported 509 cases with a matching strain and, of the cases with documented information, 80% identified themselves as MSM.
- This strain, whilst newly seen in Europe, had previously been reported in Asia and linked to an outbreak of hepatitis A in MSM in Taiwan.7
- As of 7th September 2018, a total of 4,475 outbreak-confirmed cases had been reported in 22 EU/EEA countries since 1st June 2016. Of cases where information on gender was available (4,411), the male-to-female (M/F) ratio was 6.8:1.
- Peak M/F ratio was 11.8:1, observed after May 2017.
- The most frequently reported strain was VRD_521_2016 followed by RIMV-HAV16-090 and V16-25801.
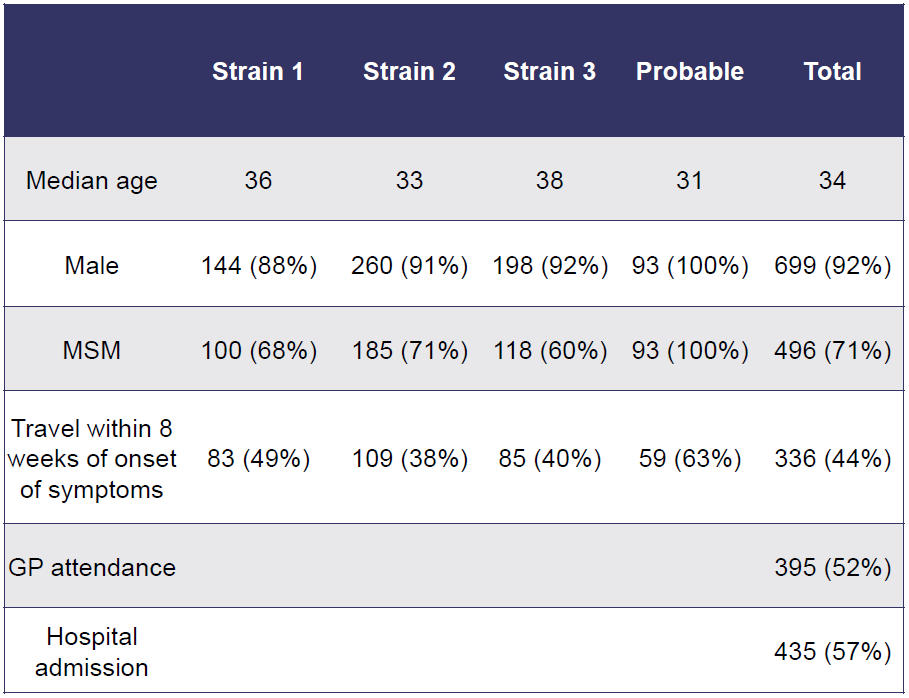
- Plunkett et al described the outbreak of hepatitis A in England between July 2016 and January 2018 (Table 1).4
- 71% of identified cases were in those identifying as MSM, potentially started with newly infected individuals returning to the UK after travel to European countries.
- Of the 1243 hepatitis A cases identified during this period, 168 (25%) were Strain 1, 287 (43%) were Strain 2 and 215 (32%) were Strain 3.
- Outbreak-associated healthcare costs were estimated to be approximately £1,500,000.
Figure 1: Strains identified from the 2016-2018 outbreak
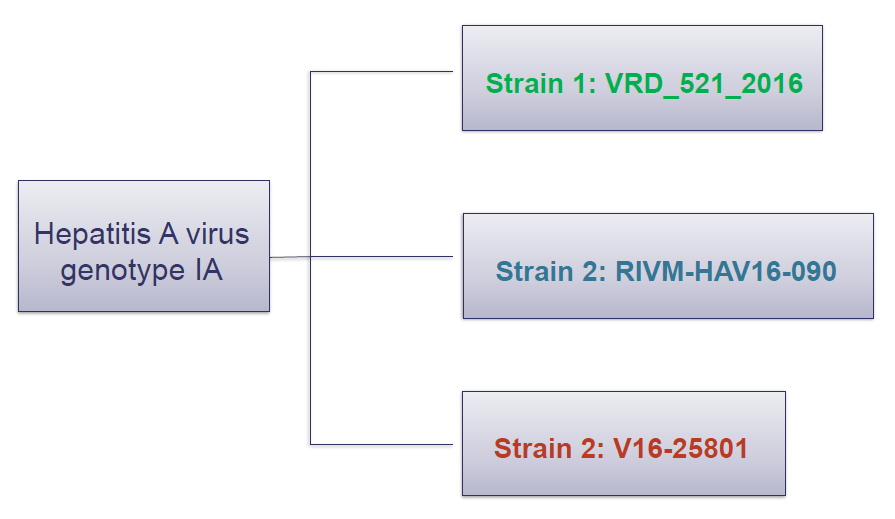
Table 1: Outbreak cases in England July 2016 to January 2018
Observations
- Sexual activity whilst abroad in the MSM cohort was assessed in a survey by the European Centre for Disease Prevention and Control in 2010:8
- The median proportion of MSM reporting sexual activity whilst abroad in the last 12 months was 26%.
- The highest reported rates were in the West (Belgium, France, Republic of Ireland, Netherlands, United Kingdom) and North-West (Denmark, Finland, Norway, Sweden) regions.
- Similarly in a study at a genitourinary medicine clinic in the UK, 44% of MSM reported a new sexual partner during their most recent trip abroad.9
Limitations
- Outbreak-confirmed cases may underestimate the actual number due to several reasons:
- Sequencing information is only available for a proportion of hepatitis A cases.
- The approach to detection varies between countries and may change depending on the different phases of the outbreak.
- Asymptomatic cases less likely to present for testing.
- Background hepatitis A immunity is not known.
Conclusions
- MSM are already identified as an at-risk group and recommendations in the UK are for MSM to be routinely offered vaccination against hepatitis A.
- As well as the prospective destination, travel health consultations routinely contain questions about planned activities and behaviours.
- In the context of hepatitis A risk in non-endemic countries, high risk sexual behaviour presents one of the most likely routes of infection.
- During an outbreak, there is a risk that the infection spreads from the MSM cohort to the wider population.
- A travel health consultation may be a useful point for opportunistic recommendation of hepatitis A vaccination in MSM in the UK, even when travel is to a non-endemic country.
- Additionally, the travel health consultation can provide a platform to discuss other preventative measures such as barrier methods during sex, personal hygiene and testing.
- Providing travel health practitioners with appropriate training and support may empower them to incorporate sexual health questions into their standard consultation.
References
- Immunisation against infectious disease: The Green Book Chapter 17. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/263309/Green_Book_Chapter_17_v2_0.pdf. Accessed 12/04/2021.
- Public Health England. Hepatitis A: guidance, data and analysis. Available: https://www.gov.uk/government/collections/hepatitis-a-guidance-data-and-analysis. Accessed 12/04/2021.
- 2017 update to the BASHH National Guidelines for the Management for Viral Hepatitides. https://www.bashhguidelines.org/media/1161/viral-hepatitides-2017-update-18-12-17.pdf. Accessed 12/04/2021
- Plunkett J (2019). Hepatitis A outbreak among men who have sex with men (MSM) in England, 2016–2018: The contribution of past and current vaccination policy and practice. Vaccine: X 1: 100014.
- European Centre for Disease Prevention and Control. Hepatitis A outbreaks in the EU/EEA mostly affecting men who have sex with men – third update, 28 June 2017. Stockholm: ECDC; 2017
- European Centre for Disease Prevention and Control. Epidemiological update: Hepatitis A outbreak in the EU/EEA mostly affecting men who have sex with men. Stockholm: ECDC; 2018
- Chen W et al. Outbreak of hepatitis A virus infection in Taiwan, June 2015 to September 2017. Euro Surveill. 2019;24(14)
- European Centre for Disease Prevention and Control EMIS 2010: The European Men-Who-Have-Sex-With-Men internet Survey.
- Hawkes S, et al. Risk behaviour and STD acquisition in genitourinary clinic attenders who have travelled. Genitourin Med 1995;71:351-354.
Conflict of Interest
This abstract was conducted and funded by Sanofi Pasteur. All authors are employees of Sanofi Pasteur, UK and may hold shares and/or stock options in the company.
Contact
Christopher Ma
Medical Advisor, Sanofi Pasteur, UK & Ireland
Christopher.Ma@Sanofi.com
Download Poster
 BACK TO TOP
BACK TO TOP
