A Stamaril Vaccine Expanded Access Investigational New Drug (IND) Program Prevented a Yellow Fever Vaccine Shortage in the United States, 2017-2020
Wayne Hachey1, Gurpreet Kaur1, Joanna Korejwo2, Andrey Rojas3, Riyadh Muhammad1
1Sanofi Pasteur, Swiftwater, USA. 2Sanofi Pasteur, Lyon, France. 3Sanofi Pasteur, Bogota, Colombia.
Download Abstract
Background
YF-VAX
- A yellow fever (YF) vaccine licensed by the United States (US) Food and Drug Administration (FDA), YF-VAX® (Sanofi Pasteur Inc., Swiftwater, PA), is a live attenuated vaccine based on strain 17D-204. It is the only YF vaccine licensed in the United States
- Due to a manufacturing disruption beginning in 2017, YF-VAX supply was not available to US civilian travel clinics. Another widely distributed YF vaccine, STAMARIL® (Sanofi Pasteur, France), was imported into the US to fulfil the public health need for YF vaccination
STAMARIL Expanded Access Investigational Program (EAP)
Stamaril vaccine is not licensed in US, therefore it is considered under FDA regulations to be an investigational product and is subject to applicable regulations under 21CFR312
Yellow Fever
- YF is a mosquito-borne hemorrhagic disease that is caused by a single-stranded RNA virus belonging to the genus Flavivirus. The virus is transmitted primarily by infected Aedes aegypti mosquitoes
- YF is widespread in sub-Saharan Africa and tropical South America and is a significant health problem to residents of endemic countries and non-vaccinated travellers entering endemic areas. There are ~200,000 cases and ~30,000 deaths due to YF worldwide each year. The case-fatality ratio varies widely in different studies but is typically 20% or higher
- Because no specific treatment exists, prevention through vaccination is critical to reduce morbidity and mortality
STAMARIL
- STAMARIL has been licensed since 1986 in more than 100 countries. Over 500 million doses have been distributed globally
- Like YF-VAX, STAMARIL is a live attenuated vaccine prepared by culturing the 17D-204 strain of yellow fever virus in chicken embryos. Vaccination provides strong and long-term protection against YF
- Safety and efficacy of STAMARIL and YF-VAX vaccines are comparable; and like all yellow fever vaccines currently available, there are three rare but important identified risks: YF vaccine-associated acute viscerotropic disease (YEL-AVD), YF vaccine-associated neurotropic disease (YEL-AND), and anaphylaxis
Methods
EAP
- To meet the public health need for a safe and effective YF vaccine for the US civilian population, in conjunction with the CDC and FDA, the EAP was implemented, allowing the importation of STAMARIL vaccine
- Typically, ~500,000 doses of YF-VAX are distributed in the US annually, with two thirds of the doses being provided to ~4,000 civilian travel clinics
- Due to the requirements of the EAP, only a limited number of clinics could participate. Approximately 250 YF vaccine clinics were enrolled as STAMARIL EAP sites based on the volume of YF-VAX previously ordered and geographic location (Figure 1). The goal was to ensure YF vaccine was available at large volume clinics and still provide geographic access to remote areas
Figure 1: Map of STAMARIL EAP sites
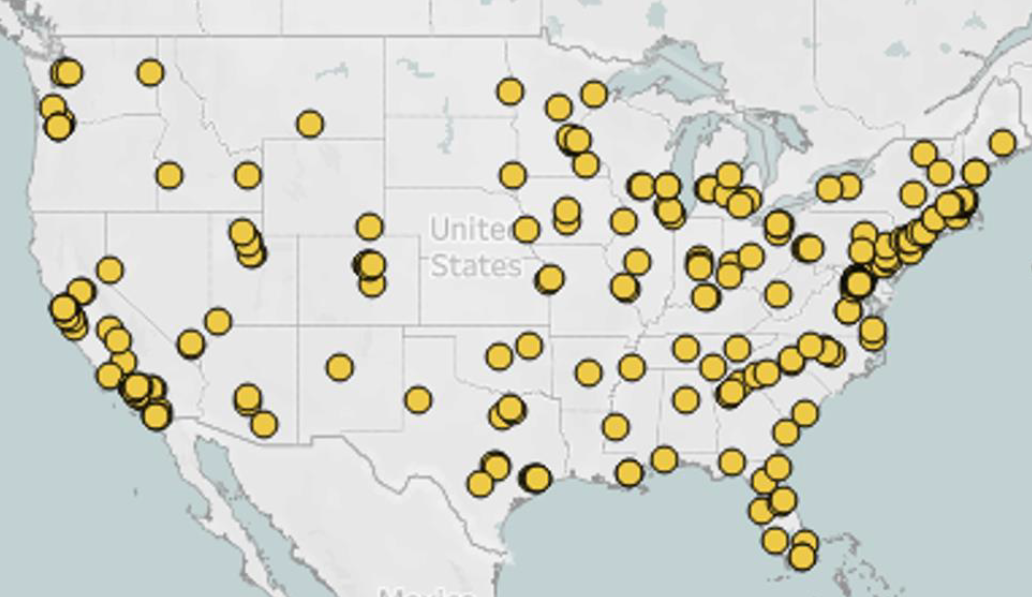
Not shown on this map are STAMARIL EAP sites in Alaska, Guam, Hawaii, Puerto Rico and the US Virgin Islands.
- Site participation required IRB approvals and adherence to protocol requirements (Table 1). Each site designated a principal investigator (YF vaccine-certified Healthcare Provider) responsible for the activities at the site and all personnel involved in the EAP completed training
- Before STAMARIL could be administered, inclusion and exclusion criteria were reviewed (Table 2), and informed consent was obtained. Participants were informed about benefits and risks of vaccination, early symptoms indicative of potential adverse reactions and instructed on how to report safety events
Table 1: EAP sites’ protocol requirements & participants process flow
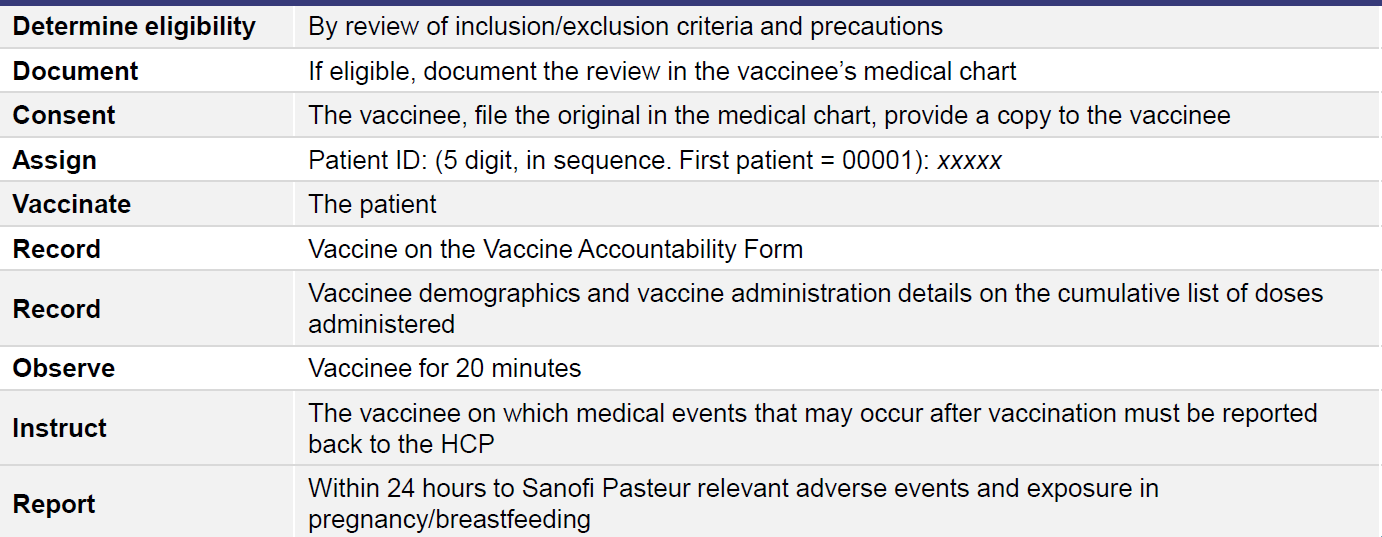
- Sites were required to report doses administered, and vaccinee demographic information
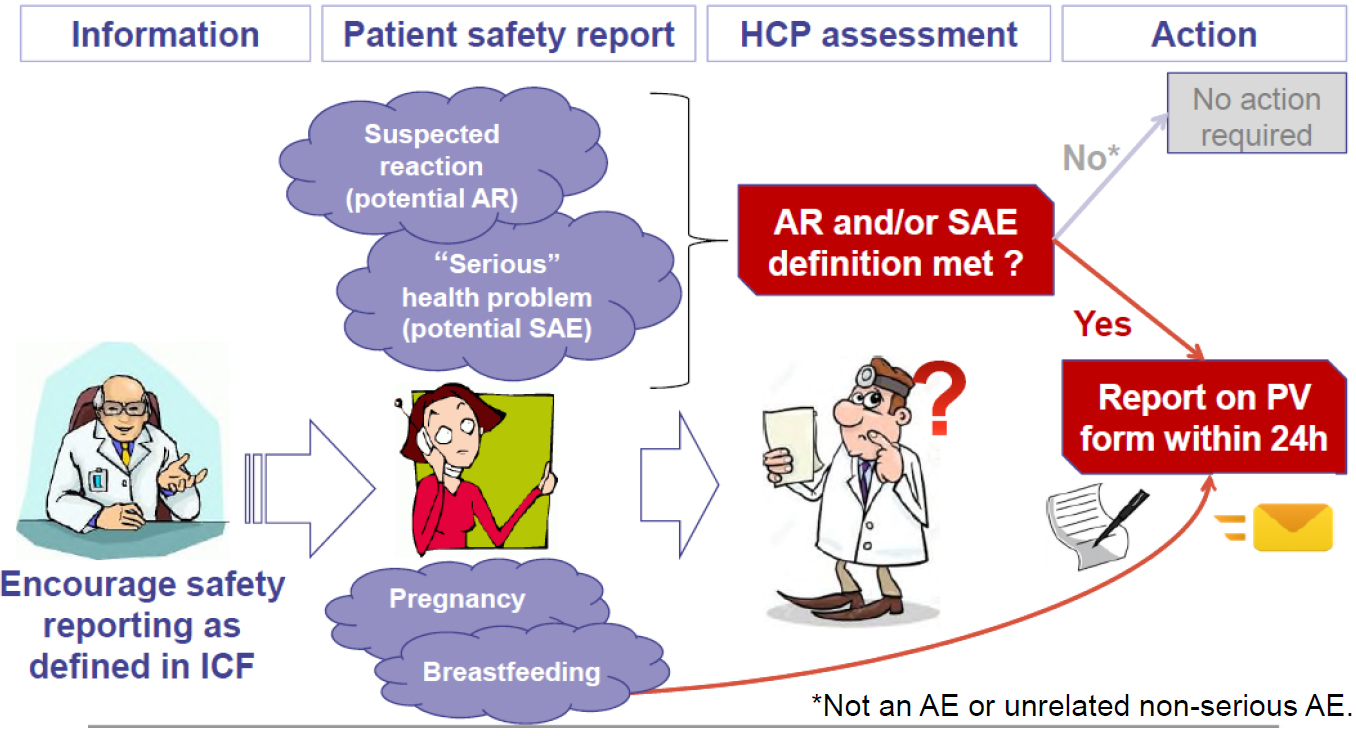
- Safety reporting required sites to inform Sanofi Pasteur within 24 hours the following: suspected adverse reactions, serious adverse events (SAEs), vaccination during pregnancy and vaccination of women who breastfed infants during the 14 days after vaccination (Figure 2)
Figure 2: Summary of Safety Reporting for the STAMARIL EAP
Results
EAP
- From May, 2017 through June, 2020, 609,010 doses of STAMARIL were administered by the EAP sites. No case of YF disease has been reported in a returning US traveler during the EAP
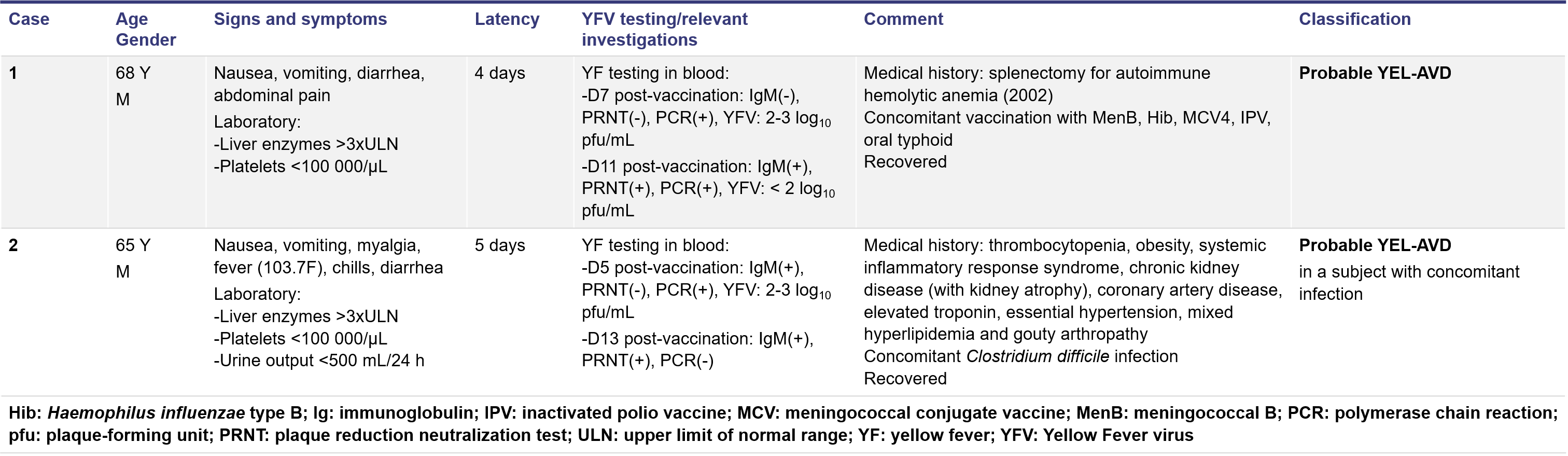
- As of December, 2020, there were seven cases of YF vaccine-associated acute neurotropic disease (YEL-AND) and two cases of YF vaccine-associated acute viscerotropic disease (YEL-AVD) reported (reporting rate: 1.1 and 0.3/100,000 vaccinees, respectively), which, with the exception of one suspect case of YEL-AND, all occurred in individuals at increased risk (age ≥ 60 years) (Tables 2-3)
- One vaccinee developed an anaphylactic reaction (reporting rate: 0.16/100,000 vaccinees)
- No safety concerns were identified from inadvertent vaccine exposure during pregnancy (41 pregnant women) or potential neonatal exposure via breast milk (4 exposed infants)
- Other relevant events included 11 reports of neurologic events not meeting the definition of YEL-AND, classified as “Level 1 neurologic disease” as per ACIP criteria. Clinical picture mainly included symptoms of aseptic meningitis, paresthesia or seizure, which started between 4 and 32 days post-vaccination. In 3 of these cases, the cerebrospinal fluid was positive for YF IgM which supported the causal association with the vaccine. These events were mainly reported in young adults, suggesting that the severity and extent of vaccine-associated neurologic reactions may be age-related
Table 2: STAMARIL EAP participant enrollment criteria
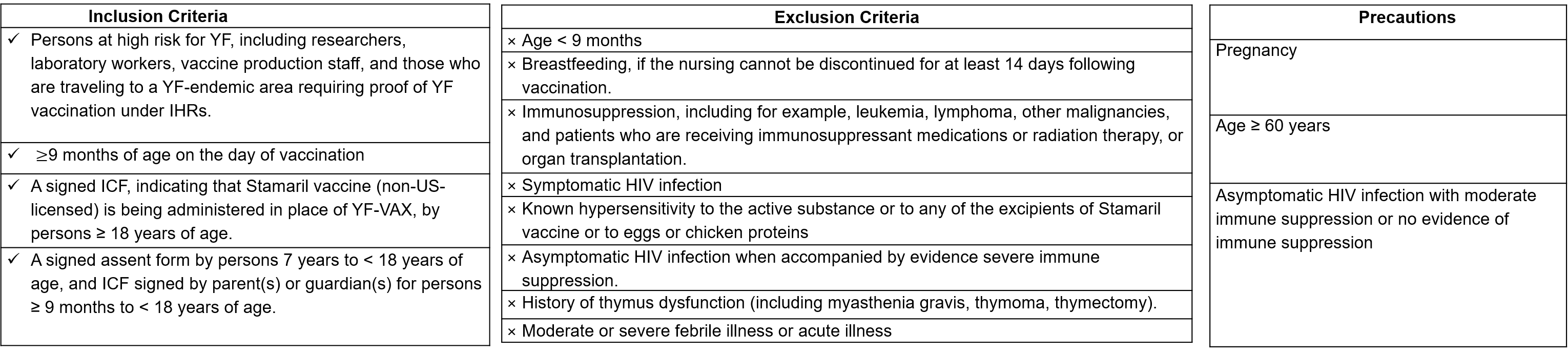
Table 3: Cases of Suspect, Probable and Definite YEL-AND reported during the EAP

Table 4: Cases of Probable YEL-AVD Reported during the EAP
Limitations
- The EAP did not include immunogenicity assessment
- EAP safety data collection was based on stimulated safety reporting (enhanced passive safety surveillance). There was no active follow-up of vaccinees for adverse events. However, underreporting of serious adverse reactions was unlikely given, the informed consent process and instructions given to all vaccinees for reporting of safety events
- Not all US travel clinics were included in the STAMARIL EAP and clinics were not randomly enrolled, thus not all travelers had similar ease of access to YF vaccination. Despite this, no cases of YF have been reported in US travelers during the EAP
Conclusions
- The STAMARIL EAP supported the public health need for YF vaccination by making an internationally licensed vaccine available to civilian travelers during the time when the US-licensed YF-VAX supply was insufficient
- For the duration of the EAP, May 2017 to present, no case of YF disease has been reported in a returning US traveler. Over 600,000 doses of STAMARIL were administered during the EAP
- No new safety concerns were identified. Serious adverse reactions remained very rare and consistent with the known safety profile of STAMARIL
- With the increase in YF-VAX manufacturing capacity and the resulting ample supply available to civilian travel, the STAMARIL EAP is anticipated to end in June 2021
References
- CDC. Yellow fever vaccine booster doses: Recommendations of the ACIP, 2015. MMWR. 2015;64(23):647-50.
- Yellow fever fact sheet. WHO Website. http://www.who.int/mediacentre/factsheets/fs100/en/. Accessed 28 April 2021.
- Yellow fever outbreak: Sanofi looks to double vaccine production. 2016. BioPharmaReporter.com Website. http://www.biopharma-reporter.com/Markets-Regulations/Yellowfever-outbreak-Sanofi-looks-to-double-vaccine-production. Accessed 28 April 2021.
- CDC. Addressing a Yellow fever vaccine shortage-United States, 2016-2017. MMWR 2017;66(17):457-59.
- CDC. Return of US licensed Yellow fever vaccine (YF-VAX) to the market. https://wwwnc.cdc.gov/travel/news-announcements/yellow-fever-vaccine-access. Accessed 28 April 2021.
Disclosures
Funding: Sanofi Pasteur
All authors are Sanofi Pasteur employees
Download Poster
 BACK TO TOP
BACK TO TOP
